Andrew Haldenby and Professor Nick Bosanquet are co-founders of Aiming for Health Success, a health research and advisory body.
Liz Truss’ instincts on public services are to devolve to strong, innovative leaders and to leave services more productive than she found them. If she can apply these calmly and consistently to the NHS, she won’t go far wrong.
She takes office in the middle of a very serious crisis in ambulance waiting times. As Steve Barclay found out last week, the public notices when performance in an essential public service collapses. Her decisions on ambulances can set the course for the rest of her health programme.
 As the chart above shows, performance on the main ambulance response time measure have been unacceptable since the spring of last year. Response times rose to over an hour in March 2022, the worst ever, and reached similar levels last month.
As the chart above shows, performance on the main ambulance response time measure have been unacceptable since the spring of last year. Response times rose to over an hour in March 2022, the worst ever, and reached similar levels last month.
The crisis in ambulance waiting times is actually a crisis in hospital occupancy due to insufficient provision of social care. Ambulances cannot be sent out while they wait outside hospitals to drop off patients. Patients cannot be dropped off if hospital beds are occupied by those unable to be discharged due to a lack of available care.
In July, around 675,000 hospital patients were judged as medically fit for discharge. Of those, 400,000 – i.e. 60 per cent – remained in hospital. No wonder ambulances are stuck.
The new Prime Minister should expect better results within weeks. The emergency need is to admit people with serious problems quickly and reduce pressures on the ambulance service. Hospitals can put up temporary accommodation to allow patients to disembark from ambulances and receive triage from an experienced consultant. Trusts can organise taxis for patients able to be discharged home, quickly followed by visits from home care teams. They can also collect data on exactly are the new patients at A&E.
Beyond the immediate emergency, hospitals can innovate. The A&E problem is not going away any time soon because of Long Covid and long waiting times, as patients can suffer crises during the wait. Hospitals under the greatest pressure need new kinds of A&E departments, incorporating teams of primary care, mental health and geriatric nurse specialists. They can treat and redirect patients who do not need emergency care. This is integrated care in action – in other words, new services that treat people more quickly and prevent them getting on the hospital waiting list in the first place.
Another key step is to fund social care better. Truss is right to seek to switch funding from the NHS to social care. It is directly in the interest of the NHS to do so. Hospitals should be able to fund care packages directly, as happened during the pandemic.
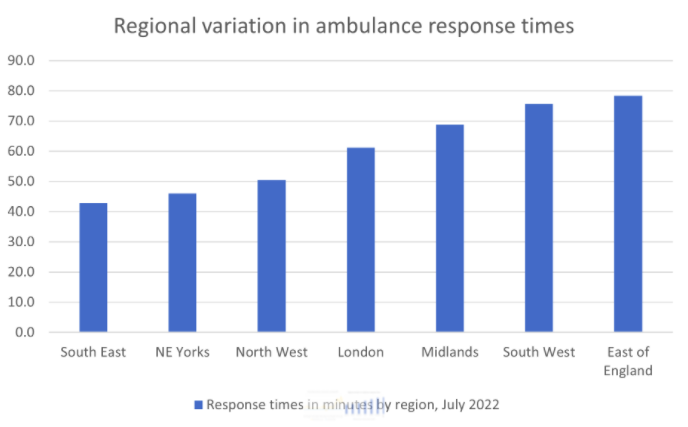
The final element is to recognise that the problem varies across the country, as do nearly all aspects of NHS performance. While the average ambulance wait in England is around an hour, actual times range from around 40 minutes in the South East to double that in the East of England.
 Rather than booming orders from the national megaphone, she needs to work directly with local leaderships to give them confidence and help them make change. A quarterly Prime Ministerial meeting with all Integrated Care System CEOs is the right kind of idea.
Rather than booming orders from the national megaphone, she needs to work directly with local leaderships to give them confidence and help them make change. A quarterly Prime Ministerial meeting with all Integrated Care System CEOs is the right kind of idea.
The new Prime Minister doesn’t need a policy revolution. The NHS is committed to the right things: much more productive hospitals, including surgical hubs; stronger out-of-hospital teams supported by new technology, community pharmacy teams and self-care; better continuity of care for high-risk patients; local leaders (integrated care systems) who can knock heads together and deliver the shift in funding from hospital to primary care.
It also has many outstanding Trust and ICS leaders who are as appalled as anyone by current levels of performance. What is needed is a step-change in speed and confidence – and much greater willingness to engage the private sector to provide treatment and support services. Her engagement can go a long way to delivering both of those things.
The final step is to signal to the NHS that it will work to these commitments for the long term – i.e: at least for this Parliament and the next. The pandemic has engendered a sense of permanent crisis, and left health leaders uncertain about Ministers’ vision. She can reassure the Service that the good Long Term Plan will remain the direction through to 2029.
On funding, her best course would be to announce a multi-year settlement of funding growth. This would allow the NHS to plan ahead and break the cycle of over-ambitious increases and freezes which have hindered service improvement for three decades. In terms of funding actual NHS organisations, she needs a payment system which incentivises two things: more productive hospitals, and better population health which reduces demand for acute care. The Treasury and the Department of Health can develop that before Christmas and implement it from April 2023 if not before.
Liz Truss can take practical steps. Restoring and then improving the NHS means getting the most from the workforce, buildings and budget that it has now. Demands for more staff (or 40 refurbished hospitals) that would materialise in ten years’ time are neither here nor there. If she engages closely with NHS leaders, she will find sympathetic people who want to deliver the virtuous circle of stronger primary care, earlier diagnosis and treatment, reduced pressure on hospitals and sustainable spending. She has every chance of succeeding.
Andrew Haldenby and Professor Nick Bosanquet are co-founders of Aiming for Health Success, a health research and advisory body.
Liz Truss’ instincts on public services are to devolve to strong, innovative leaders and to leave services more productive than she found them. If she can apply these calmly and consistently to the NHS, she won’t go far wrong.
She takes office in the middle of a very serious crisis in ambulance waiting times. As Steve Barclay found out last week, the public notices when performance in an essential public service collapses. Her decisions on ambulances can set the course for the rest of her health programme.
The crisis in ambulance waiting times is actually a crisis in hospital occupancy due to insufficient provision of social care. Ambulances cannot be sent out while they wait outside hospitals to drop off patients. Patients cannot be dropped off if hospital beds are occupied by those unable to be discharged due to a lack of available care.
In July, around 675,000 hospital patients were judged as medically fit for discharge. Of those, 400,000 – i.e. 60 per cent – remained in hospital. No wonder ambulances are stuck.
The new Prime Minister should expect better results within weeks. The emergency need is to admit people with serious problems quickly and reduce pressures on the ambulance service. Hospitals can put up temporary accommodation to allow patients to disembark from ambulances and receive triage from an experienced consultant. Trusts can organise taxis for patients able to be discharged home, quickly followed by visits from home care teams. They can also collect data on exactly are the new patients at A&E.
Beyond the immediate emergency, hospitals can innovate. The A&E problem is not going away any time soon because of Long Covid and long waiting times, as patients can suffer crises during the wait. Hospitals under the greatest pressure need new kinds of A&E departments, incorporating teams of primary care, mental health and geriatric nurse specialists. They can treat and redirect patients who do not need emergency care. This is integrated care in action – in other words, new services that treat people more quickly and prevent them getting on the hospital waiting list in the first place.
Another key step is to fund social care better. Truss is right to seek to switch funding from the NHS to social care. It is directly in the interest of the NHS to do so. Hospitals should be able to fund care packages directly, as happened during the pandemic.
The final element is to recognise that the problem varies across the country, as do nearly all aspects of NHS performance. While the average ambulance wait in England is around an hour, actual times range from around 40 minutes in the South East to double that in the East of England.
The new Prime Minister doesn’t need a policy revolution. The NHS is committed to the right things: much more productive hospitals, including surgical hubs; stronger out-of-hospital teams supported by new technology, community pharmacy teams and self-care; better continuity of care for high-risk patients; local leaders (integrated care systems) who can knock heads together and deliver the shift in funding from hospital to primary care.
It also has many outstanding Trust and ICS leaders who are as appalled as anyone by current levels of performance. What is needed is a step-change in speed and confidence – and much greater willingness to engage the private sector to provide treatment and support services. Her engagement can go a long way to delivering both of those things.
The final step is to signal to the NHS that it will work to these commitments for the long term – i.e: at least for this Parliament and the next. The pandemic has engendered a sense of permanent crisis, and left health leaders uncertain about Ministers’ vision. She can reassure the Service that the good Long Term Plan will remain the direction through to 2029.
On funding, her best course would be to announce a multi-year settlement of funding growth. This would allow the NHS to plan ahead and break the cycle of over-ambitious increases and freezes which have hindered service improvement for three decades. In terms of funding actual NHS organisations, she needs a payment system which incentivises two things: more productive hospitals, and better population health which reduces demand for acute care. The Treasury and the Department of Health can develop that before Christmas and implement it from April 2023 if not before.
Liz Truss can take practical steps. Restoring and then improving the NHS means getting the most from the workforce, buildings and budget that it has now. Demands for more staff (or 40 refurbished hospitals) that would materialise in ten years’ time are neither here nor there. If she engages closely with NHS leaders, she will find sympathetic people who want to deliver the virtuous circle of stronger primary care, earlier diagnosis and treatment, reduced pressure on hospitals and sustainable spending. She has every chance of succeeding.