Alexander Bowen is an MPP-MIA student at SciencesPo Paris and St Gallen specialising in public health.
In December, New Zealand’s new government scrapped its smokefree generation strategy – the plan to ratchet up the minimum age of purchase annually until nobody can legally purchase tobacco.
Yet two months prior, directly inspired by Wellington’s approach, Rishi Sunak announced that exact same policy having been recommended it a year prior.
New Zealand’s abrupt change of course should give ministers a chance to, as the slogan goes, stop and think. Though I strongly support stronger public health measures, the Government must be wary of this one for a simple reason: the evidence base, or at least its interpretation of it, has major flaws.
The core problem? The baseline scenario, i.e. what is projected would happen if the rising age limit were not introduced, and against which the policy’s projected success is assessed.
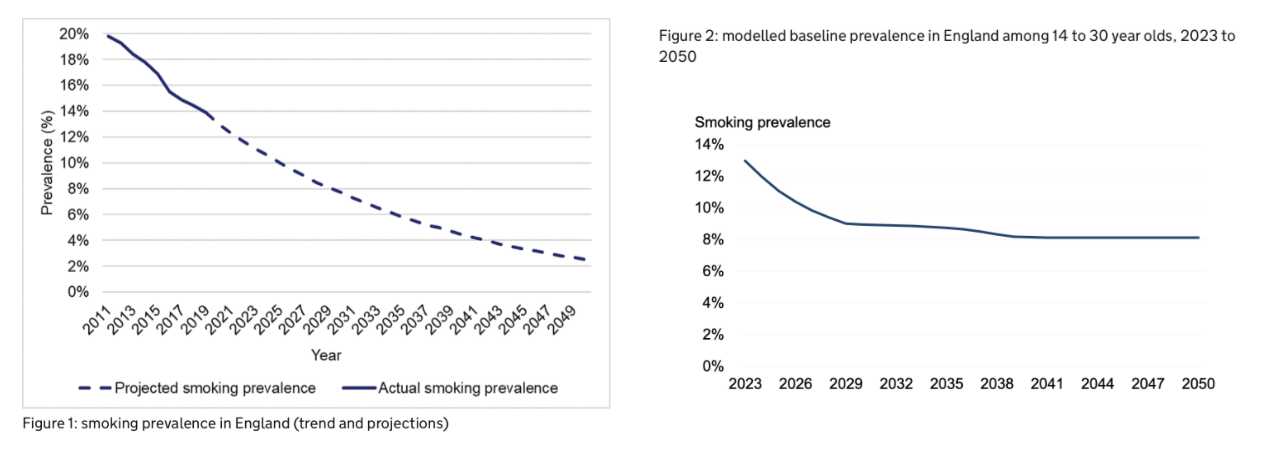
The baseline used in the Government’s model foresees smoking prevalence falling from 13 per cent in 2023 to nine per cent in 2030 before essentially flatlining at little more than eight percent until at least 2050 (Fig 2 below).
However, this baseline scenario is an order of magnitude different to the baseline scenario in the original review calling for the policy. The Khan Review’s projection was that today’s 13 per cent smoking prevalence would fall to two per cent by 2050 (Fig 1).
I make no comment on which baseline is more accurate, but the stark difference between the two is certainly odd to say the least. It could be noted though that the Khan Review’s projections are rather more in line with independent third-party projections including that of Cancer Research UK, those of the Belgium government, and those from New Zealand.
(An eagle eye-observer might spot that these figures represent marginally different demographics. But given the 18-24 year old age group is the second least likely to smoke, there is little reason to believe this accounts for a noticeable part of the difference.)
Why the difference in these baselines matter is that by modelling a drop to zero per cent from an eight per cent baseline (which is what three of the four scenarios consider) the policy appears to be at least 400 percent more effective than it would have on the Khan Review’s two percent to zero per cent figure.
If this new baseline were wrong, both the assessed health and economic benefits of the policy would be greatly inflated. It would thus be useful to know where this new baseline originated and what it was based on.
Yet not only is this not explained, nowhere in the modelling website’s explanation of how it came to its baseline are the Khan Review’s different projections even acknowledged. More weirdly still, it references both Cancer Research UK and the Royal College of Physicians’ projections, claiming that the Government’s new baseline is “in line with other published estimates”.
But these projections are actually an order of magnitude different to the Government’s (and much more in line with Khan’s).
Next, there’s the question of compliance. As anyone passingly familiar with drugs policy or the history of alcohol prohibition will tell you, it’s one thing to ban something, but quite another to actually prevent people using it.
Yet in three of the four scenarios used to assess the new policy’s impact, the percentage of current smokers drops to zero. That’d be an astonishing and well-worthwhile achievement, but how do they think it will happen? Is it even remotely plausible to predict getting smoking to zero at all?
The modellers reach this remarkable outcome by modelling the impact if the initiation rate (that is the odds of starting smoking) were to fall by 30 percent, 60 percent, or 90 percent. Yet all these scenarios are fundamentally static: they assume that falls in initiation simply compound. You burn through the modelled smokers as people quit, fewer start, and demographics shift, until you reach zero (and if it were allowed to go below zero, below zero).
A neat model certainly. But in the real world compliance is not a static; it is always marginal, subject to real-world confounders and diminishing returns.
Given 2.5 percent of people age 11-15, and five percent of 15 year olds, already smoke despite it being illegal, and something like nine percent of secondary school pupils do illicit drugs monthly, there seem little grounds for assuming a new smoking age will be totally successful when existing prohibitions are not.
This is especially so as the primary enforcement mechanism proposed is merely to give councils more power to fine retailers – a policy which has not stamped out the existing trade in under-the-counter cigarettes or underage purchase of alcohol.
New Zealand was much more realistic about what achieving compliance would involve: Jacinda Ardern’s government planned to shut down 95 percent of tobacco retail points, vaguely akin to creating a tobacco equivalent of Norway’s state alcohol monopoly, to add barriers to access and ease enforcement.
There is nothing of this in Sunak’s proposals which amount to creating a half-way house between legal tobacco and illegal weed. (This is to say nothing of New Zealand’s innate advantage in terms of stopping smuggled tobacco entering its market.)
In fact, the Prime Minister has copied the least effective strand of the previous New Zealand government’s approach, as well as the hardest one to enforce. In Wellington’s modelling, the smokefree generation plan, if implemented without the other parts of their three-pronged package, accounted for only 12 percent of the total anticipated gains in terms of Health Adjusted Life Years (HALYs) saved by the package as a whole (HALYs being similar to QALYs, with which Sunak is well familiar).
Meanwhile the aggressive shuttering of tobacco retailers accounted for 19 percent, whilst 97 percent of gains could come from de-nicontinisation alone (forcing manufacturers to slash nicotine levels in cigarettes, a practice with precedence in the UK and EU).
Tightening regulations on manufacturers, ideally in partnership with the EU, might not grab any headlines. But if it works, isn’t that what matters?
On the subject of compliance, it’s also worth noting that policy on tobacco seems to be running in a fashion that is completely contrary to that on drugs such as marijuana, despite the fact that the arguments for legalisation – hundreds of millions in tax revenue, harm-reduction, combating crime – are identical for each.
Now none of this is enough to say that phasing out the legal purchase of tobacco is conclusively bad per sé; frankly, I do not think we know enough either way.
It is however sufficient grounds to demand that MPs subject it, and the evidence offered by ministers to support it, to rigorous scrutiny.
Though it might not be fashionable to do so, fully scrutinising legislation is Parliament’s moral obligation. Good intentions do not make good policy, even when we’re talking tobacco.
It would be a dereliction of its duty if Parliament were to wave through a policy (which, unlike New Zealand, would almost certainly never be repealed) that risks being fundamentally flawed from the get-go and is both less practical and less effective than alternative strategies (denicotinisation, anyone?).
Smoking is a catastrophe for both individual and public health. Yet rushed policy generally can do just as much harm in the long run – and, sadly, seems almost as addictive to politicians as nicotine.
Alexander Bowen is an MPP-MIA student at SciencesPo Paris and St Gallen specialising in public health.
In December, New Zealand’s new government scrapped its smokefree generation strategy – the plan to ratchet up the minimum age of purchase annually until nobody can legally purchase tobacco.
Yet two months prior, directly inspired by Wellington’s approach, Rishi Sunak announced that exact same policy having been recommended it a year prior.
New Zealand’s abrupt change of course should give ministers a chance to, as the slogan goes, stop and think. Though I strongly support stronger public health measures, the Government must be wary of this one for a simple reason: the evidence base, or at least its interpretation of it, has major flaws.
The core problem? The baseline scenario, i.e. what is projected would happen if the rising age limit were not introduced, and against which the policy’s projected success is assessed.
The baseline used in the Government’s model foresees smoking prevalence falling from 13 per cent in 2023 to nine per cent in 2030 before essentially flatlining at little more than eight percent until at least 2050 (Fig 2 below).
However, this baseline scenario is an order of magnitude different to the baseline scenario in the original review calling for the policy. The Khan Review’s projection was that today’s 13 per cent smoking prevalence would fall to two per cent by 2050 (Fig 1).
I make no comment on which baseline is more accurate, but the stark difference between the two is certainly odd to say the least. It could be noted though that the Khan Review’s projections are rather more in line with independent third-party projections including that of Cancer Research UK, those of the Belgium government, and those from New Zealand.
(An eagle eye-observer might spot that these figures represent marginally different demographics. But given the 18-24 year old age group is the second least likely to smoke, there is little reason to believe this accounts for a noticeable part of the difference.)
Why the difference in these baselines matter is that by modelling a drop to zero per cent from an eight per cent baseline (which is what three of the four scenarios consider) the policy appears to be at least 400 percent more effective than it would have on the Khan Review’s two percent to zero per cent figure.
If this new baseline were wrong, both the assessed health and economic benefits of the policy would be greatly inflated. It would thus be useful to know where this new baseline originated and what it was based on.
Yet not only is this not explained, nowhere in the modelling website’s explanation of how it came to its baseline are the Khan Review’s different projections even acknowledged. More weirdly still, it references both Cancer Research UK and the Royal College of Physicians’ projections, claiming that the Government’s new baseline is “in line with other published estimates”.
But these projections are actually an order of magnitude different to the Government’s (and much more in line with Khan’s).
Next, there’s the question of compliance. As anyone passingly familiar with drugs policy or the history of alcohol prohibition will tell you, it’s one thing to ban something, but quite another to actually prevent people using it.
Yet in three of the four scenarios used to assess the new policy’s impact, the percentage of current smokers drops to zero. That’d be an astonishing and well-worthwhile achievement, but how do they think it will happen? Is it even remotely plausible to predict getting smoking to zero at all?
The modellers reach this remarkable outcome by modelling the impact if the initiation rate (that is the odds of starting smoking) were to fall by 30 percent, 60 percent, or 90 percent. Yet all these scenarios are fundamentally static: they assume that falls in initiation simply compound. You burn through the modelled smokers as people quit, fewer start, and demographics shift, until you reach zero (and if it were allowed to go below zero, below zero).
A neat model certainly. But in the real world compliance is not a static; it is always marginal, subject to real-world confounders and diminishing returns.
Given 2.5 percent of people age 11-15, and five percent of 15 year olds, already smoke despite it being illegal, and something like nine percent of secondary school pupils do illicit drugs monthly, there seem little grounds for assuming a new smoking age will be totally successful when existing prohibitions are not.
This is especially so as the primary enforcement mechanism proposed is merely to give councils more power to fine retailers – a policy which has not stamped out the existing trade in under-the-counter cigarettes or underage purchase of alcohol.
New Zealand was much more realistic about what achieving compliance would involve: Jacinda Ardern’s government planned to shut down 95 percent of tobacco retail points, vaguely akin to creating a tobacco equivalent of Norway’s state alcohol monopoly, to add barriers to access and ease enforcement.
There is nothing of this in Sunak’s proposals which amount to creating a half-way house between legal tobacco and illegal weed. (This is to say nothing of New Zealand’s innate advantage in terms of stopping smuggled tobacco entering its market.)
In fact, the Prime Minister has copied the least effective strand of the previous New Zealand government’s approach, as well as the hardest one to enforce. In Wellington’s modelling, the smokefree generation plan, if implemented without the other parts of their three-pronged package, accounted for only 12 percent of the total anticipated gains in terms of Health Adjusted Life Years (HALYs) saved by the package as a whole (HALYs being similar to QALYs, with which Sunak is well familiar).
Meanwhile the aggressive shuttering of tobacco retailers accounted for 19 percent, whilst 97 percent of gains could come from de-nicontinisation alone (forcing manufacturers to slash nicotine levels in cigarettes, a practice with precedence in the UK and EU).
Tightening regulations on manufacturers, ideally in partnership with the EU, might not grab any headlines. But if it works, isn’t that what matters?
On the subject of compliance, it’s also worth noting that policy on tobacco seems to be running in a fashion that is completely contrary to that on drugs such as marijuana, despite the fact that the arguments for legalisation – hundreds of millions in tax revenue, harm-reduction, combating crime – are identical for each.
Now none of this is enough to say that phasing out the legal purchase of tobacco is conclusively bad per sé; frankly, I do not think we know enough either way.
It is however sufficient grounds to demand that MPs subject it, and the evidence offered by ministers to support it, to rigorous scrutiny.
Though it might not be fashionable to do so, fully scrutinising legislation is Parliament’s moral obligation. Good intentions do not make good policy, even when we’re talking tobacco.
It would be a dereliction of its duty if Parliament were to wave through a policy (which, unlike New Zealand, would almost certainly never be repealed) that risks being fundamentally flawed from the get-go and is both less practical and less effective than alternative strategies (denicotinisation, anyone?).
Smoking is a catastrophe for both individual and public health. Yet rushed policy generally can do just as much harm in the long run – and, sadly, seems almost as addictive to politicians as nicotine.